
Salt Substitute Potassium Risk Calculator
Calculate Your Potassium Risk
Estimate daily potassium intake from salt substitutes and check if you're at risk when taking ACE inhibitors or ARBs.
Many people switch to salt substitutes thinking they’re making a healthy choice-especially if they’re trying to lower their blood pressure. But for those taking ACE inhibitors or ARBs, that seemingly harmless swap could be dangerous. These substitutes often replace sodium chloride with potassium chloride, and when combined with certain blood pressure medications, they can push potassium levels in your blood to life-threatening levels. This isn’t a rare side effect. It’s a quiet, widespread risk that many patients don’t even know about.
What Are Salt Substitutes, Really?
Salt substitutes are marketed as healthier alternatives to regular table salt. Products like LoSalt, NoSalt, and Heart Salt contain anywhere from 25% to 100% potassium chloride instead of sodium chloride. A typical "lite" salt blend is half sodium, half potassium. Pure substitutes like LoSalt are about 66% potassium chloride. That means one teaspoon of these products can deliver 400-600 mg of potassium, compared to almost none in regular salt.
On the surface, this sounds good. Potassium helps relax blood vessels and lower blood pressure. The American Heart Association recommends reducing sodium to under 2,300 mg a day, and many people consume over 3,400 mg daily-mostly from processed foods. So swapping salt for a potassium-based version seems like a win. But here’s the catch: your kidneys need to work well to get rid of extra potassium. If they’re not functioning properly, potassium builds up.
Why ACE Inhibitors and ARBs Are a Problem
ACE inhibitors (like lisinopril, enalapril) and ARBs (like losartan, valsartan) are among the most common medications for high blood pressure, heart failure, and kidney protection in diabetics. They work by blocking the renin-angiotensin-aldosterone system (RAAS), which helps regulate blood pressure and fluid balance. One of the side effects? Reduced aldosterone production-by 30% to 50%. Aldosterone tells your kidneys to excrete potassium. Less aldosterone means less potassium leaves your body.
Now add potassium-rich salt substitutes on top of that. Your body is taking in more potassium while simultaneously losing the ability to flush it out. This double hit can cause hyperkalemia-dangerously high potassium levels in the blood. Levels above 5.0 mmol/L are considered elevated. Above 6.5 mmol/L, you risk cardiac arrest. A 2004 case report in the Journal of the Royal Society of Medicine documented a 72-year-old patient who suffered cardiac arrest after using LoSalt while on nabumetone and with mild kidney impairment. His potassium level hit 7.8 mmol/L.
Who’s at Highest Risk?
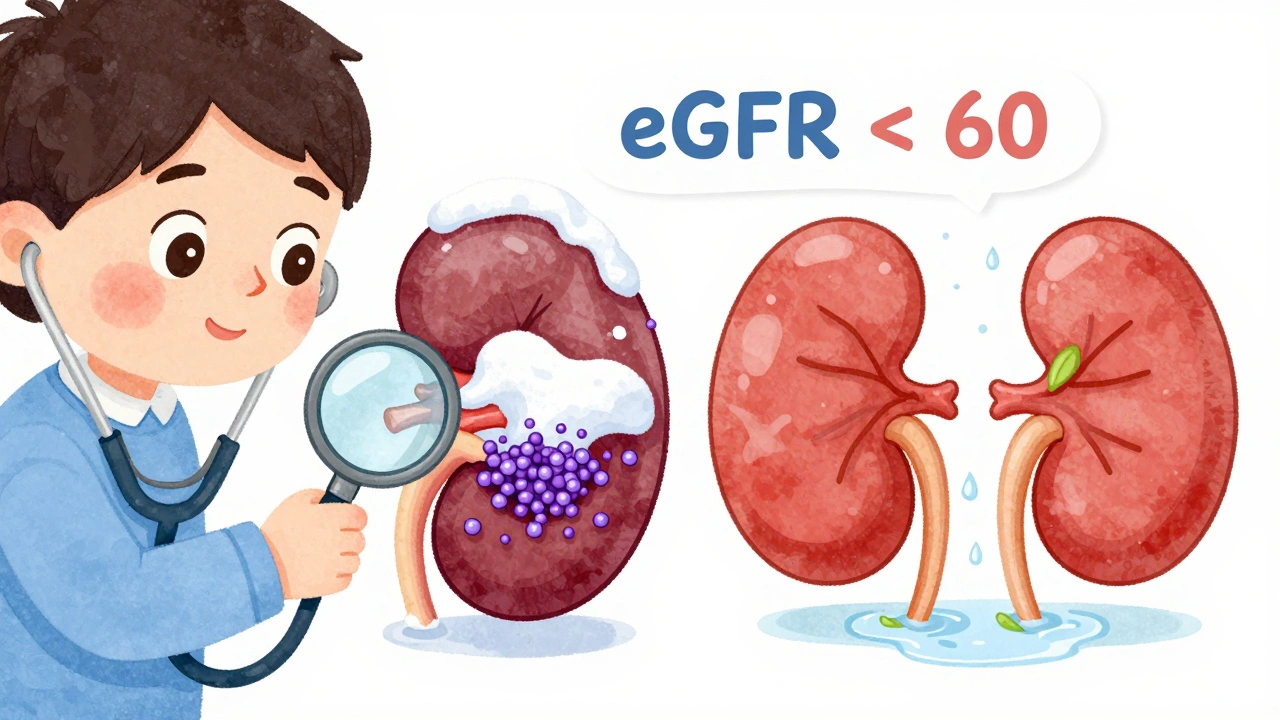
The biggest risk group isn’t just people on these medications-it’s people on these medications and with kidney problems. About 15% of U.S. adults have chronic kidney disease (CKD), according to CDC 2022 data. That’s roughly 37 million people. Of those, about 14.5% have an estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73m², meaning their kidneys can’t efficiently remove potassium.
Diabetics are especially vulnerable. Up to 20% of diabetics with kidney disease have hyporeninemic hypoaldosteronism-a condition where the body makes even less aldosterone. The American Diabetes Association specifically warns that this group faces a "disproportionately high" risk of hyperkalemia when using potassium salt substitutes.
Even if you don’t know you have kidney disease, you might still be at risk. Many people with early-stage CKD feel fine. No swelling. No fatigue. Just quietly declining kidney function. That’s why screening matters.
The Numbers Don’t Lie
Research shows how serious this is. A 2019 meta-analysis of over 1.2 million people found that hyperkalemia occurred at a rate of 0.8 events per 100 person-years in the general population using salt substitutes. But for those with CKD and on ACE inhibitors or ARBs? That jumped to 8.7 events per 100 person-years-more than ten times higher.
And it’s not just theory. Reddit threads, Drugs.com reviews, and Amazon feedback are full of stories: "Woke up in the ER with potassium at 6.3 after using Heart Salt for 3 weeks on lisinopril." "Severe muscle weakness and irregular heartbeat after switching to potassium salt while on losartan." These aren’t outliers. They’re predictable outcomes.
Meanwhile, a 2025 JAMA Network study showed potassium-enriched salt substitutes reduced stroke recurrence by 14% in 21,000 people with normal kidney function. But that study excluded people with eGFR under 60. The benefits? Real. The risks? Real too. It’s not a one-size-fits-all solution.
What About Other Ways to Cut Salt?
You don’t need potassium chloride to lower sodium. Herbs, spices, citrus, vinegar, garlic, and onion powder can reduce sodium intake by 40-50% without any potassium risk. Products like Mrs. Dash are sodium-free and potassium-free. They don’t have that metallic aftertaste that 28% of users complain about in Amazon reviews. They’re cheaper, too-most cost under $3 for a 12-ounce container, compared to $5-$6 for potassium-based substitutes.
And here’s the thing: most of the sodium in your diet comes from packaged and restaurant foods-not the salt shaker. Cutting back on processed snacks, canned soups, deli meats, and frozen meals does more than any salt substitute ever could. A 2022 Mayo Clinic study found that 63% of hyperkalemia cases in people on ACE inhibitors or ARBs came from dietary potassium sources like salt substitutes, not supplements.
What Should You Do?
If you’re on an ACE inhibitor or ARB, here’s what to do right now:
- Check your salt substitute. Look at the ingredient label. If it says "potassium chloride," stop using it.
- Ask your doctor for a blood test. Get your serum potassium level checked. Normal is 3.5-5.0 mmol/L. Anything above 5.0 needs attention.
- Know your kidney function. Ask for your eGFR. If it’s below 60, avoid potassium substitutes entirely.
- Switch to herbs and spices. Use garlic, paprika, cumin, lemon zest, black pepper, and dried herbs to flavor food. They work.
- Don’t assume "low sodium" means safe. Many low-sodium products replace sodium with potassium. Read labels like a detective.
The National Kidney Foundation and American Society of Hypertension now recommend that doctors ask every patient on ACE inhibitors or ARBs about salt substitute use at every visit. Yet a 2023 JAMA Internal Medicine study found that 78% of patients on these drugs didn’t even know dietary potassium could be dangerous.
The Bigger Picture
The global salt substitute market is growing fast-projected to hit $2.3 billion by 2030. But regulation lags. In the U.S., the FDA doesn’t require warning labels on potassium salt substitutes for people on ACE inhibitors or ARBs. Canada did-starting January 2024. Only 3 out of 12 major brands in the U.S. voluntarily warn about this risk.
The FDA proposed new labeling rules in May 2024, but they won’t be final until at least mid-2026. Until then, the burden is on you and your doctor.
Final Thought: It’s Not About Fear-It’s About Awareness
Reducing sodium is important. Managing blood pressure saves lives. But if you’re on an ACE inhibitor or ARB, potassium salt substitutes aren’t a shortcut-they’re a trap. The good news? You don’t need them. You can still eat flavorful, heart-healthy food without touching a single gram of potassium chloride.
Talk to your doctor. Get tested. Switch to herbs. Your heart-and your kidneys-will thank you.
Can I use salt substitutes if I’m on lisinopril?
If you’re on lisinopril or any ACE inhibitor, avoid salt substitutes that contain potassium chloride. These can cause your potassium levels to rise dangerously high, leading to heart rhythm problems or cardiac arrest. Stick to potassium-free seasoning blends like Mrs. Dash, herbs, spices, or citrus instead.
What are the symptoms of high potassium?
Symptoms of hyperkalemia include muscle weakness, numbness or tingling, nausea, irregular heartbeat, chest pain, and in severe cases, sudden cardiac arrest. Many people have no symptoms until potassium levels are dangerously high, which is why blood tests are critical if you’re on ACE inhibitors or ARBs.
Is potassium chloride in salt substitutes the same as potassium supplements?
Yes, chemically, potassium chloride in salt substitutes is the same compound used in potassium supplements. The difference is in how it’s delivered: supplements are taken in controlled doses, while salt substitutes can be used freely in cooking, leading to unintentional overconsumption. Both can raise blood potassium levels, especially when combined with ACE inhibitors or ARBs.
How often should I get my potassium checked if I’m on an ACE inhibitor?
If you’re on an ACE inhibitor or ARB and have normal kidney function, your doctor may check potassium once or twice a year. If you have kidney disease (eGFR under 60) or are using potassium salt substitutes, check every 3 months. Always get tested before starting or stopping any potassium-containing product.
Are there any salt substitutes that are safe for people on blood pressure meds?
Yes-salt substitutes that contain no potassium chloride. Look for products labeled "potassium-free" or check the ingredients: if it only lists herbs, spices, or sodium-free seasonings (like Mrs. Dash), they’re safe. Avoid anything with "potassium chloride," "KCl," or "potassium" in the ingredients list.
Why don’t more people know about this risk?
Because the marketing for salt substitutes focuses on lowering sodium, not the hidden potassium risk. Labels rarely warn about interactions with ACE inhibitors or ARBs. Doctors don’t always ask about dietary habits. And patients assume "natural" or "heart-healthy" means safe. This knowledge gap is why so many end up in the ER.

13 Comments
Jamie Clark
Let’s be real-this isn’t about salt. It’s about how we outsource our health decisions to marketing departments and then wonder why we’re in the ER. They slap "heart-healthy" on a bag of potassium chloride and suddenly we’re heroes for avoiding sodium. Meanwhile, our kidneys are screaming into a void while our doctors are too busy to ask about seasoning. This is systemic negligence dressed up as wellness.
Michael Gardner
Actually, the real problem is that people think potassium is some magical nutrient. It’s not. It’s just another electrolyte. Too much of it kills you just like too much sodium. The fact that we treat it like a superfood while ignoring the dose-response curve is why medicine is so broken.
Willie Onst
Man, I love this post. Seriously. I’m from Texas, grew up on salted everything, and switched to Mrs. Dash after my dad had a scare. No more weird metallic taste, no more panic attacks over potassium levels. Just garlic, smoked paprika, and a squeeze of lime. Food tastes better when it’s not trying to kill you. Thanks for putting this out there-it’s the kind of info that saves lives, not just clicks.
nina nakamura
You missed the point. The FDA doesn’t regulate this because they’re in bed with the food industry. Potassium chloride is cheaper than herbs. They’d rather you die quietly than lose a profit margin. Also, if you’re on an ACE inhibitor and using salt substitutes, you’re not just dumb-you’re negligent. Get tested or stop pretending you care about your health.
Rawlson King
Canada implemented labeling in 2024. The U.S. still hasn’t. That’s not oversight. That’s a death sentence written in bureaucratic delay. People don’t die from salt substitutes-they die because corporations and regulators decided profit mattered more than transparency.
Constantine Vigderman
OMG YES!! I just found out my mom was using LoSalt on her pasta and she’s on lisinopril 😱 I had no idea!! I told her to stop immediately and we got her potassium checked-6.1!! She’s in the hospital now but alive bc we caught it. Thank you for this post!! I’m telling everyone!! 🙏❤️
Cole Newman
Wait so you’re telling me I can’t use that fancy pink salt I bought on Amazon? I thought it was all natural and shit. My wife’s on valsartan and I’ve been using it for months. Are we gonna die? Should I panic? Like right now? I’m sweating.
Casey Mellish
As an Australian who’s seen this play out in our public health system, I can confirm: the risk is real and grossly undercommunicated. We had a cluster of hyperkalemia cases in rural Queensland last year-all linked to potassium salt substitutes sold as "healthy alternatives" in pharmacies. The solution isn’t fear. It’s education. And labeling. And doctors asking the right questions. Simple. Effective. Neglected.
Emily Haworth
🚨 THIS IS A BIG PHARMA COVER-UP 🚨
They don’t want you to know that potassium chloride is a slow poison disguised as wellness. The FDA’s delay? Totally intentional. They’re waiting for enough people to die so they can launch a "new safety initiative" and profit from the panic. Look at the patents. Look at the lobbyists. Look at the timing. This isn’t negligence. It’s genocide by bureaucracy. 💀🩸
Tom Zerkoff
Thank you for this meticulously researched and clinically significant contribution. The confluence of pharmacological mechanisms, epidemiological data, and behavioral health gaps presented here represents a critical public health imperative. I urge all clinicians to incorporate structured dietary potassium screening into routine hypertension management protocols. Furthermore, I recommend that patient education materials be standardized across primary care networks to include explicit warnings regarding potassium chloride-containing products in the context of RAAS inhibition. This is not merely advisory-it is foundational to patient safety.
Yatendra S
Interesting. But tell me-why do we assume that replacing sodium with potassium is inherently better? Isn’t that just another form of reductionism? Nature doesn’t work in binaries. Maybe the real issue is our obsession with replacing one chemical with another instead of eating whole foods. Salt is just a symptom. The disease is industrialized eating.
Himmat Singh
While the empirical data presented is compelling, it is imperative to acknowledge that the causal inference drawn between potassium chloride consumption and hyperkalemia may be confounded by concomitant renal dysfunction and medication adherence variability. Furthermore, the exclusion criteria of the 2025 JAMA study render its generalizability questionable in populations with comorbid conditions. A more nuanced approach to dietary intervention is warranted.
kevin moranga
Look, I get it. This stuff is scary. But here’s the good news-you don’t have to be perfect. You don’t have to throw out every spice jar and start from scratch. Start small. Swap out one thing this week. Use garlic powder instead of that potassium salt. Try lemon juice on your eggs. Maybe skip the canned soup and make your own. It’s not about being a saint-it’s about being aware. And if you’re on meds, talk to your doctor. Not tomorrow. Today. I’ve seen too many people wait until they’re in the ER. You don’t have to be one of them. You got this. One spice at a time. 💪